Skeleton and Movement
Can you recall? Page No. 193
1. Which are different types of muscular tissues ?
Answer: The different types of muscular tissues are smooth muscles, cardiac muscles, and striated (skeletal) muscles.
2. Name the type of muscles which bring about running and speaking.
Answer: Striated (skeletal) muscles bring about running and speaking, as they control voluntary movements.
3. Name the muscles which do not contract as per of our will.
Answer: Smooth muscles and cardiac muscles do not contract as per our will, as they are involuntary.
4. Which types of muscles show rhythmic contractions?
Answer: Cardiac muscles show rhythmic contractions, controlling the heart’s beating.
5. Which type of muscle is present in the diaphragm of the respiratory system?
Answer: Striated (skeletal) muscle is present in the diaphragm, allowing voluntary control during breathing.
6. Name the part of human skeleton situated along the vertical axis.
Answer: The axial skeleton, including the skull, vertebral column, and thoracic cage, is situated along the vertical axis.
Think about it Page No. 193
1. Why do we shiver during winter ?
Answer: Shivering occurs in winter as skeletal muscles contract rapidly and involuntarily to generate heat through muscle activity, helping to maintain body temperature in cold conditions.
2. Why do muscles show spasm after rigourous contraction?
Answer: Muscles show spasms after rigorous contraction due to the accumulation of lactic acid from anaerobic metabolism, causing fatigue and temporary disruption in muscle relaxation, leading to involuntary contractions.
3. Did you ever feel tickling in muscles?
Answer: The document does not directly address the sensation of tickling in muscles, but this feeling may occur due to nerve irritation or minor muscle contractions, often linked to fatigue or stimulation of sensory nerves in the muscle tissue.
Can you tell? Page No. 194
1. Why are movement and locomotion necessary among animals?
Answer: Movement and locomotion are necessary among animals to search for food, find shelter, locate mates, reach breeding grounds, and escape from predators, ensuring survival and reproduction.
2. Differentiate between :
Answer:
a. Flexor and Extensor Muscles
- Flexor Muscles: These muscles contract to bend or flex a joint, reducing the angle between bones, e.g., biceps flex the elbow.
- Extensor Muscles: These muscles contract to straighten or extend a joint, increasing the angle between bones, e.g., triceps extend the elbow.
b. Pronator and Supinator
- Pronator Muscles: These muscles rotate the forearm to turn the palm downward, e.g., pronator teres.
- Supinator Muscles: These muscles rotate the forearm to turn the palm upward, e.g., supinator muscle.
3. What are antagonistic muscles? Explain with example.
Answer: Antagonistic muscles are pairs of muscles that produce opposite actions at a joint, working together to control movement. For example, the biceps (flexor) and triceps (extensor) in the upper arm are antagonistic; the biceps contract to bend the elbow, while the triceps contract to straighten it, ensuring coordinated movement.
Can you tell? Page No. 197
1. Why are muscle rich in creatine phosphate?
Answer: Muscles are rich in creatine phosphate because it serves as a rapid energy reserve, quickly transferring phosphate to ADP to regenerate ATP, which is essential for muscle contraction during short bursts of intense activity.
2. What do you understand by muscle twitch?
Answer: A muscle twitch is a single, brief contraction and relaxation of a muscle fiber initiated by a single electrical stimulus, consisting of a latent period (no contraction), a contraction period, and a relaxation period.
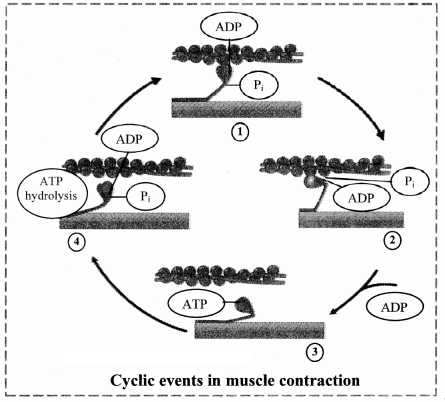
3. Explain mechanism of muscle contraction and relaxation.
Answer:
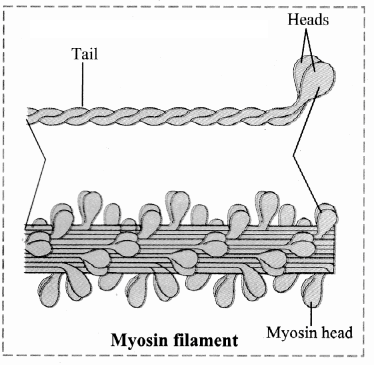
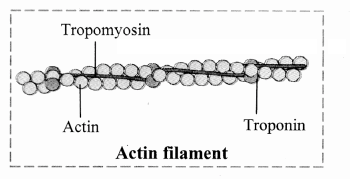
- Contraction: A nerve impulse triggers the release of calcium ions from the sarcoplasmic reticulum, which bind to troponin, shifting tropomyosin to expose actin’s binding sites. Myosin heads, energized by ATP hydrolysis, bind to actin, forming cross-bridges, and tilt to pull actin filaments inward, shortening the sarcomere.
- Relaxation: When stimulation stops, calcium is pumped back into the sarcoplasmic reticulum using ATP, allowing the troponin-tropomyosin complex to cover actin’s binding sites again. Myosin detaches from actin (using ATP), and actin filaments slide back, relaxing the muscle.
4. Explain the chemical changes taking place in muscle contraction.
Answer: During muscle contraction, ATP is hydrolyzed by myosin heads to ADP and inorganic phosphate, releasing energy for cross-bridge formation and the power stroke, pulling actin filaments. Calcium ions bind to troponin, triggering a conformational change in tropomyosin to expose actin’s binding sites. In relaxation, ATP is used to pump calcium back into the sarcoplasmic reticulum and detach myosin from actin, restoring the resting state.
Do you remember? Page No. 198
1. What are the components of our skeletal system ?
Answer: The skeletal system consists of bones, cartilage, and exoskeletal structures like nails, horns, hooves, scales, and hair, with bones and cartilage forming the major endoskeletal components.
2. What type of bones are present in our body?
Answer: The human body contains long bones (e.g., femur), short bones (e.g., carpals), flat bones (e.g., skull), irregular bones (e.g., vertebrae), and sesamoid bones (e.g., patella).
3. How do bones help us in various ways ?
Answer: Bones provide structural support and shape to the body, protect delicate organs (e.g., skull protects the brain), facilitate movement through joints, serve as attachment sites for muscles, store calcium, and act as sites for hematopoiesis (blood cell formation).
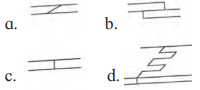
Identify and label Page No. 199
Identify the different bones.
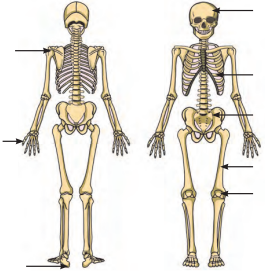
Answer:
Use your brain power Page No. 199
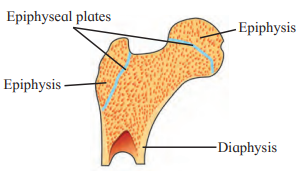
Why are long bones slightly bent and not straight ?
Answer: Long bones are slightly bent and not straight to distribute weight and stress more evenly across their structure, enhancing their strength and flexibility to withstand mechanical forces during movement and weight-bearing activities.
Can you tell? Page No. 201
1. Give schematic plan of human skeleton.
Answer: The human skeleton consists of 206 bones, divided into two main divisions:
- Axial Skeleton (80 bones): Includes the skull (22 bones: 8 cranium, 14 facial), hyoid bone (1), ear ossicles (6), vertebral column (26: 7 cervical, 12 thoracic, 5 lumbar, 1 sacrum, 1 coccyx), and thoracic cage (25: 1 sternum, 24 ribs).
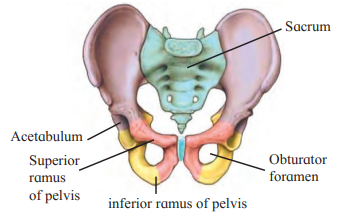
- Appendicular Skeleton (126 bones): Comprises the pectoral girdle (4: 2 clavicles, 2 scapulae), upper limbs (60: 2 humerus, 2 radius, 2 ulna, 16 carpals, 10 metacarpals, 28 phalanges), pelvic girdle (2: 2 coxal bones), and lower limbs (60: 2 femur, 2 patella, 2 tibia, 2 fibula, 14 tarsals, 10 metatarsals, 28 phalanges).
2. Enlist the bones of cranium.
Answer: The bones of the cranium are:
- Frontal bone (unpaired)
- Parietal bones (paired)
- Temporal bones (paired)
- Occipital bone (unpaired)
- Sphenoid bone (unpaired)
- Ethmoid bone (unpaired)
3. Write a note on structure and function of skull.
Answer:
- Structure: The skull comprises 22 bones, divided into the cranium (8 bones) and facial bones (14 bones). The cranium includes the frontal, parietal, temporal, occipital, sphenoid, and ethmoid bones, forming a protective brain box with sutures (immovable joints) like coronal, sagittal, lambdoidal, and lateral/squamous. Facial bones, such as the maxilla, mandible, nasals, and zygomatic, shape the face, with the mandible being the only movable bone. The skull also includes features like the foramen magnum (for spinal cord passage) and sella turcica (for pituitary gland).
- Function: The skull protects the brain, supports sensory organs (e.g., eyes, ears), provides attachment sites for muscles of the head and neck, and forms the framework for the face, contributing to identity and functions like chewing and speech. It also houses sinuses to lighten the skull and aid voice resonance.
Can you Tell? Page No. 202
Why skull is important for us? Enlist few reasons.
Answer: The skull is crucial for several reasons:
- It protects the brain from injury, ensuring the safety of this vital organ.
- It provides structural support and shape to the face, contributing to individual identity.
- It houses sensory organs (e.g., eyes, ears) and supports functions like vision and hearing.
- It serves as an attachment site for muscles involved in head movement, chewing, and speech.
- It contains sinuses that lighten the skull and aid in voice resonance.
Try this Page No. 202
Feel your spine (vertebral column). Is it straight or curved?
Answer: The vertebral column is not straight; it has four curvatures: cervical and lumbar curves (secondary, convex) and thoracic and sacral curves (primary, concave). These curvatures help maintain balance in an upright position, absorb shocks during walking, and protect vertebrae from fracture.
Can you tell? Page No. 204
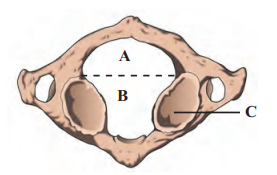
1. Explain the structure of a typical vertebra.
Answer: A typical vertebra consists of a prominent central body called the centrum, which is flat in the anteroposterior aspect (amphiplatyan). Posterior to the centrum, two short, thick processes unite to form the neural arch, creating a vertebral foramen that surrounds the spinal cord. The neural arch extends into a spinous process (neural spine) for muscle attachment. Transverse processes project laterally from the neural arch for muscle attachment. Superior and inferior zygapophyses (articular processes) on either side allow articulation with adjacent vertebrae, and intervertebral foramina at their junctions permit passage of spinal nerves.
2. How will you identify a thoracic vertebra?
Answer: A thoracic vertebra can be identified by its heart-shaped centrum and well-developed processes. It has facets on the transverse processes (except for vertebrae 11 and 12) for articulation with ribs, and the centrum has demifacets for rib attachment. These features, along with its location in the chest region, distinguish it from other vertebrae.
3. Write a note on curvatures of vertebral column and mention their importance.
Answer: The vertebral column has four curvatures: cervical and lumbar (secondary, convex, developing after birth) and thoracic and sacral (primary, concave, present at birth). These curvatures maintain balance in an upright posture, distribute mechanical stress evenly, and absorb shocks during walking or other activities. They also protect the vertebrae from fracture and enhance the spine’s flexibility and resilience.
Can you recall? Page No. 206
How does humerus form ball and socket joint? Where is it located ?
Answer: The humerus forms a ball and socket joint through its hemispherical head at the proximal end, which fits into the glenoid cavity of the scapula, a concave socket in the pectoral girdle. This structure allows multiaxial movements, including flexion, extension, abduction, adduction, and rotation. The joint is located at the shoulder, connecting the upper arm to the axial skeleton.
Can you tell? Page No. 208
1. Differentiate between skeleton of palm and foot.
Answer:
| Skeleton of palm | Skeleton of foot | |
| a. | It consists of metacarpals and phalanges | It consists of metatarsals and phalanges |
| b. | Saddle joints and condyloid joints are in the palm. | Condyloid or saddle joints are not present the foot. |
2. Explain the longest bone in human body.
Answer: The femur, located in the thigh, is the longest bone in the human body. It has a head connected to the shaft by a short neck, forming a ball and socket joint with the acetabulum of the coxal bone at the hip. The shaft’s lower third forms a triangular popliteal surface, and the distal end has two condyles that articulate with the tibia and fibula, supporting weight-bearing and movement.
Do you remember? Page No. 208
1. What are joints? What are their types?
Answer: Joints, also known as articulations or arthroses, are points where two or more bones meet, enabling movement and flexibility. They are classified based on the degree of movement into three types:
- Synarthroses (Fibrous Joints): Immovable, held by fibrous connective tissue, e.g., sutures (skull), syndesmoses (tibiofibular ligament), gomphoses (teeth in jaw).
- Amphiarthroses (Cartilaginous Joints): Slightly movable, connected by hyaline or fibrocartilage, e.g., synchondroses (epiphyseal plate), symphysis (intervertebral discs, pubic symphysis).
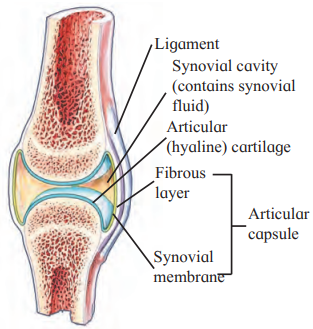
- Diarthroses (Synovial Joints): Freely movable, with a synovial cavity, hyaline cartilage, and synovial fluid, e.g., pivot (atlas-axis), ball and socket (shoulder), hinge (elbow), condyloid (metacarpophalangeal), saddle (thumb), gliding (intercarpal).
2. What types of joint is present at knee?
Answer: The knee joint is a hinge joint, a type of synovial joint that allows monoaxial movement, primarily flexion and extension, between the femur and tibia.
Use your brain power Page No. 210
Why are warming up rounds essential before regular exercise?
Answer: Warming up rounds are essential before regular exercise because they increase blood flow to muscles, raise muscle temperature, and reduce the viscosity of synovial fluid in joints, thereby enhancing flexibility, improving performance, and preventing injuries.
Can you tell? Page No. 211
1. Human beings can hold an object in a better manner than monkeys. Why?
Answer: Human beings can hold objects better than monkeys due to the presence of a saddle joint at the carpometacarpal joint of the thumb, which allows for greater flexibility and precision in movements like opposition, abduction, and circumduction. This joint, characteristic of Homo sapiens, enables a stronger and more precise grip compared to monkeys, whose thumb joints are less specialized for such fine motor tasks. Additionally, humans have more developed fine motor control and dexterity due to advanced neural coordination.
3. What makes the synovial joint freely moveable?
Answer: Synovial joints are freely movable due to the presence of a synovial cavity filled with synovial fluid, which lubricates the joint and reduces friction. The articulating surfaces are covered with hyaline cartilage, which minimizes wear and absorbs shocks, while the synovial membrane and ligaments (including the fibrous capsule) provide stability without restricting movement. These features collectively allow a wide range of motions, such as flexion, extension, rotation, and circumduction, depending on the joint type.